Amy from New York
Severe MTHFR
 We are proud to introduce our daughter, Amy, to this group and hope that there might be some things that people read that can be useful in the treatment of their children. She was born on February 28th, 2008, thereby avoiding a potential Leap Year birthday. Now, as a 15-year-old about to go to the public high school that her older brother graduated from and where her older sister is going to be a senior, Amy is a tall, pretty, artistic, fashion-loving young woman, who is painfully shy at first but is by nature very sweet. Her face lights up when she hears that we are going to be in the presence of any of a number of babies in our family. Once she started being tested/examined by experts, she showed a toughness and bravery which she doesn’t always give herself credit for, but that we remind her of constantly.
We are proud to introduce our daughter, Amy, to this group and hope that there might be some things that people read that can be useful in the treatment of their children. She was born on February 28th, 2008, thereby avoiding a potential Leap Year birthday. Now, as a 15-year-old about to go to the public high school that her older brother graduated from and where her older sister is going to be a senior, Amy is a tall, pretty, artistic, fashion-loving young woman, who is painfully shy at first but is by nature very sweet. Her face lights up when she hears that we are going to be in the presence of any of a number of babies in our family. Once she started being tested/examined by experts, she showed a toughness and bravery which she doesn’t always give herself credit for, but that we remind her of constantly.
Unlike most of the other Homocystinuria families that we have connected with, Amy did not receive her diagnosis of Homocystinuria due to severe MTHFR deficiency until she was almost 15 years old. Unfortunately, there was no newborn screening done for severe MTHFR deficiency, which is not on the recommended list of diseases to screen for. Amy is the third child in our family, our baby, and her brother and sister are neurotypical, healthy teenagers (ages 17 and 19). My pregnancies were normal, except for gestational diabetes, which I had during all three pregnancies. The diabetes was well controlled by insulin, and the children were unaffected at birth.
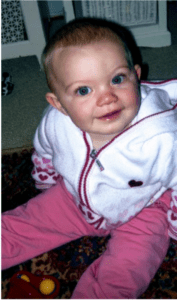
 Amy was a happy baby, who appeared to be on the same track in terms of developmental milestones until she reached about two years. When my mother expressed concern for her development, I made excuses by pointing out that Amy was often put in and out of the stroller/ car seat while we ran around to her siblings’ daily activities, and rarely took a nap at home in the crib. Similarly, I attributed her delayed speech to having her needs met by her siblings’ requests. After attending half day nursery school at the ages of two and three, she was recommended for early intervention speech services at the age of 4, which she received twice weekly until she was declassified going into kindergarten. Amy was happy in kindergarten, but her teacher expressed concerns about her ability to recognize basic numbers, letters, colors and we noticed that she struggled with coordination. She also struggled with her sense of time, and the ability to remember anything sequential: days of the week, months, or words to songs. In the first grade she was tested by the school district and was offered speech therapy twice a week. Amy also began to struggle socially, as friends and classmates naturally became more discriminating and as friends embraced and excelled at sports and dance activities that were too challenging for her. When we witnessed a group of her peers chatting at social gatherings, it seemed that the pace of their conversation was too fast and in time their interests grew further apart.
Amy was a happy baby, who appeared to be on the same track in terms of developmental milestones until she reached about two years. When my mother expressed concern for her development, I made excuses by pointing out that Amy was often put in and out of the stroller/ car seat while we ran around to her siblings’ daily activities, and rarely took a nap at home in the crib. Similarly, I attributed her delayed speech to having her needs met by her siblings’ requests. After attending half day nursery school at the ages of two and three, she was recommended for early intervention speech services at the age of 4, which she received twice weekly until she was declassified going into kindergarten. Amy was happy in kindergarten, but her teacher expressed concerns about her ability to recognize basic numbers, letters, colors and we noticed that she struggled with coordination. She also struggled with her sense of time, and the ability to remember anything sequential: days of the week, months, or words to songs. In the first grade she was tested by the school district and was offered speech therapy twice a week. Amy also began to struggle socially, as friends and classmates naturally became more discriminating and as friends embraced and excelled at sports and dance activities that were too challenging for her. When we witnessed a group of her peers chatting at social gatherings, it seemed that the pace of their conversation was too fast and in time their interests grew further apart.
We applied to a specialty private school for language-based learning disabilities and had to do some private testing with a neuropsychologist for her application. One neurologist suggested that she might be having “mini-seizures” when it appeared that she was staring into space. She had an abnormal EEG in the office, showing micro-seizures when provoked, but a 72-hour video EEG was normal. She continued to walk with severe “in-toeing” but the pediatric orthopedic thought she would grow out of it. Similarly, her pediatrician was unconcerned.
Amy attended a private school from second grade through ninth grade which had extremely small class sizes, modified curriculum, and assessments. Amy had a lot of social anxiety and would get sick almost every morning before school. She took medication for ADD and the anti-anxiety medication which was very helpful and resolved her morning stomach issues. We continued to have her IEP done by the public school of record throughout her time at the private school, in case they thought she was ready to return to the public school so that she would at least receive the tri-annual testing. She was classified as Learning Disabled at this time.
small class sizes, modified curriculum, and assessments. Amy had a lot of social anxiety and would get sick almost every morning before school. She took medication for ADD and the anti-anxiety medication which was very helpful and resolved her morning stomach issues. We continued to have her IEP done by the public school of record throughout her time at the private school, in case they thought she was ready to return to the public school so that she would at least receive the tri-annual testing. She was classified as Learning Disabled at this time.
In April of 2020, Amy had her first focal seizure while on a walk with her dad. She collapsed and was staring at the sky and was unresponsive to her dad’s attempt to get her attention. After about 3-4 minutes, she came to, and he was able to support her enough to get her home. She was diagnosed with epilepsy and began taking Keppra to control the seizures.
We also had her tested for autism, and she was diagnosed with that in 2021. A few months later she had another seizure during which only half of her body was seizing. There is some debate among her doctors as to whether this was actually a stroke. Around this time her unusual gate became more pronounced. In early 2022 we did genetic testing and learned about the Severe MTHFR deficiency. Her homocysteine level was over 200. It is better controlled now, with her numbers between 70-80. However, in May of 2023, Amy told us that she was having trouble seeing and that she was seeing “dots”. After a visit to a retina specialist, we were told that her optic nerve was swollen and that we should take her to the ER. She ended up having a spinal tap to relieve the intracranial hypertension. Amy is now taking Diamox to prevent further buildup of excess fluid. It is hard to pinpoint what caused the excess cerebrospinal fluid; it could have been a side effect of the medications she takes, her genetic condition, or related to being overweight. She now also wears AFO braces on her feet, receives botox injections in her legs and hips and physical therapy to help with her gait disorder.
This spring Amy also received eligibility through the OPWDD (Office for People with Developmental Disabilities) and is currently attending her first camp program for individuals with disabilities. She will be in a similar program at our public high school this fall. Dropping her off at camp with teenagers and young adults with Downs Syndrome, autism and other physical and developmental conditions was a new experience for us. Given that her progressive condition and resulting cognitive decline has occurred mostly in the last few years, we didn’t know how she would feel about being with new people, some with more obvious physical challenges and some almost ten years older than she. After a month of camp, it seems like it has been a good experience for her. She talks about having friends, and for the first time in a long time, she describes being good at things, even helping other campers. While this makes us very happy, it also reminds us that it must have been painful for her to have struggled to keep up with others - physically and mentally - in a typical classroom for so long.
We knew nothing about Homocystinuria or Severe MTHFR deficiency. Most of her doctors don’t know much about it either, and I’m not even sure if anyone does newborn screening for it in NY. For many years we treated her symptoms in isolation, having no idea that a genetic test could provide an answer for us. It is upsetting to think that if we had known to get her tested sooner, and if we had started treatment at a much younger age, she might be in a very different situation at this time. We have a letter from her geneticist that we carry with us in the event she is in an emergency room, as well as a list of all of her medications, so that we can explain her condition to the doctors on call.
 It is hard to write about how having a child with special needs impacts the entire family, although the effects are considerable. It is particularly challenging given the fact that this could be read by any of our family members, and we don’t want any one of us to feel culpable in any way. As parents, we know that having a child with special needs can be isolating, and we have experienced anger and frustration at our situation. We struggle to practice patience, with our children and ourselves, knowing that we are all experiencing a sense of loss. Our other children have had to be independent, and while ultimately this may benefit them in some ways, losing time with parents because they are busy with caretaking and the logistics that come with frequent therapies and doctors’ appointments will no doubt have impacted them, as being independent and being forced to be independent are very different situations. Amy’s sister, Kiera, suffers from AMPS (Amplified Musculoskeletal Pain Syndrome) which was also diagnosed through genetic testing, and fibromyalgia, which we want to mention in the event that there is a connection between the two genetic conditions. Having more than one child with medical issues is something that also appears to be common in families with metabolic genetic disorders.
It is hard to write about how having a child with special needs impacts the entire family, although the effects are considerable. It is particularly challenging given the fact that this could be read by any of our family members, and we don’t want any one of us to feel culpable in any way. As parents, we know that having a child with special needs can be isolating, and we have experienced anger and frustration at our situation. We struggle to practice patience, with our children and ourselves, knowing that we are all experiencing a sense of loss. Our other children have had to be independent, and while ultimately this may benefit them in some ways, losing time with parents because they are busy with caretaking and the logistics that come with frequent therapies and doctors’ appointments will no doubt have impacted them, as being independent and being forced to be independent are very different situations. Amy’s sister, Kiera, suffers from AMPS (Amplified Musculoskeletal Pain Syndrome) which was also diagnosed through genetic testing, and fibromyalgia, which we want to mention in the event that there is a connection between the two genetic conditions. Having more than one child with medical issues is something that also appears to be common in families with metabolic genetic disorders.

Fortunately, we are blessed with family and friends, who help with driving to appointments, financial assistance (co-pays and parking in Manhattan where she has had more than 20 appointments in the past year adds up!) and many who have helped us by listening. Even though it must be irritating when our conversations with friends inevitably involve discussing our latest medical news, it helps us process what is happening and just listening helps more than they know.
We are so proud of Amy, as well as her siblings, Kiera and Brendan. If a hero is someone who combats adversity with strength, they have ALL shown remarkable heroism in the face of this challenging situation. Amy is our HCU hero because she demonstrates strength on a daily basis when she takes her medicine and suffers from its side effects without complaint. She hasaccepted her condition with grace and by example, teaches us to practice patience and inclusivity.